Let me congratulate everyone gastoenterology-addicted with our professional holiday!
пятница, 29 мая 2009 г.
Endoscopy: Biliary Tract. Photodynamic therapy for cholangiocarcinoma. Part 1
Part 1
 By Norman E. Mar con
By Norman E. Mar conDivision of Gastroenterology The Wellesley Hospital Site, University of Toronto
160 Wellesley Street East Toronto, Ontario M4Y 1J3, Canada
Tel.: +1-4.16-926-7763, fax: +1-416-926-4951
Bile duct carcinoma is an uncommon malignant tumor, which occurs more frequently in the elderly. Several predisposing factors include ulcerative colitis, sclerosing cholangitis, an anomalous long pancreatic biliary channel, Clonorchis sinensis infestation, and possibly transduodenal sphincterotomy for benign disease.
Biliary carcinoma is traditionally classified as occurring in the lower third (intrapancreatic portion), middle third (from the cystic duct to the superior border of the pancreas) or upper third (the common hepatic duct and confluence of the right and left hepatic ducts). About 35% of the lesions arise in the middle or lower third, and diffuse types account for 10%, whereas 55% occur in the upper third. Bismuth and Corlette (Surg Gynecol Obstet 1975; 140:170) described patterns of tumor involvement of the proximal biliary system. In type I, the cancer extends to, but does not involve, the bifurcation; in type II, the cancer involves the bifurcation but does not extend into either hepatic duct; type III (a and b) involves the bifurcation and unilateral hepatic duct, without extension into secondary radicles on either the right or left side; and type IV extends up into the secondary radicals bilaterally.
Tumors of the middle and distal third of the bile duct often cause biliary obstruction when they are quite small, and if operable are usually well served by resection. In contrast, cancers of the proximal third may involve predominantly the right or left hepatic duct, allowing drainage through the uninvolved duct, thereby preventing clinical jaundice until the tumors either become locally advanced or metastatic. Surgery with excision of the tumor and intrahepatic bile ducts often requires hepatic and vascular resection. In one series, a survival after resection aiming at "cure" was 66% at one year and 26% at five years (Klempnauer et al. J Clin Oncol 1997; 15:947). In those who underwent palliative surgical bypass, the one-year and five-year survival rates were 21% and 2%, respectively Since the procedure-related morbidity and mortality is significantly lower using endoscopic methods, insertion of either a plastic or metal stent is the method of choice for palliation. Although metal stent placement results in higher patency, the survival time is not increased compared to that with plastic endoprostheses.
Technical success, with effective drainage, is achieved in 91 %, with a median survival time of 149 days in Bismuth type I and 84 days for type II (Polydo-rou etal. Grot 1991; 32:685, Ducreux et al. Dig Dis Sci 1992; 37:778). In type III, the drainage results are tragically poor, with a 30-day mortality of 32% and a median survival of only 70 days (Bismuth et al. Ann Surg 1992; 215:31). These studies demonstrate that stenting fails to prolong the relief of jaundice and the symptoms of pruritus, anorexia, diarrhea, and altered sleep pattern. These failures are reflected by a poor performance status on the Karnofsky index or QLQ-C 30 (quality-of-life questionnaire).
There is therefore a great deal of scope for improvement. Ortner et al. (1998) bring a fresh outlook, with the application of photodynamic therapy (PDT) using the photosensitizer Photo-frin. In summary, she and her colleagues treated nine patients with Bismuth III and IV cholangiocarcinoma in whom plastic stent insertion failed to produce an adequate improvement in drainage. After intraluminal PDT, the bilirubin level fell significantly in all patients. This was associated with a significant improvement in the Karnofsky score and no mortalities within 30 days, with a median survival time of 439 days. In two patients, no further stent placement was required after PDT ablation.
What is PDT? It is a unique treatment modality involving the use of an instrument (a laser) and a photosensitive drug. Although PDT has been clinically used in the gastrointestinal tract since the early 1980s, it did not achieve wide acceptance in the gastroenterology community until the last five years, and then it was mainly for the treatment of various stages of cancer in the esophagus (Lightdale et al. Gast-rointest Endose 1995; 42:307,
Sibille et al. Gastroenterology 1995; 108:537). The sensitizer is activated by applying laser light in the red spectrum (630 nm). The only photosensitizer commercially available, and with widespread regulatory approval, is Photofrin (porfimer, dihemato-porphyrin ether) (QLT, Vancouver, Canada). With this drug and laser wavelength, destruction into the tumor is 3-5 mm. Laser light is delivered directly to the tumor via a diffusing fiber passed through a trans-sphincteric or percutaneous miniscope. A photochemical reaction (light plus drug) results in the release of locally toxic singlet oxygen, which destroys the microvascu-lature of the tumor, resulting in necrosis, sloughing, and hopefully improved lumen patency. If the tumor is superficial, PDT may be curative, as in the esophagus (Gossner et al. Gast-
roenterology 1998; 114:448).
In the study by Ortner et al., nine patients had not responded with a decrease in jaundice, despite presumably adequately placed stents through and above the stenosis. They received Photofrin (2 mg/kg i.v.), and 48 hours later the stent was removed and intraluminal photoactivation using an argon dye laser (wavelength 630 nm, 310mW/cm2, 180j/cm2) treatment was carried out using diffusing tips of 2-5 cm or 4 cm. The laser light was delivered via a mother/daughter system through the baby scope channel. These fibers have a metallic tip to facilitate placement under fluoroscopic control. The light exposure time for treatment was only between 10 and 16 minutes. Immediately after the light treatment, the plastic stents were replaced.

вторник, 26 мая 2009 г.
Endoscopy: Gl Tract. Ablating Barrett's mucosa
 By: S.C. Sydney Chung
By: S.C. Sydney ChungCorresponding address: S.C. Sydney Chung, M.D.
Prince of Wales Hospital, Department of Surgery Shatin, New Territories, Hong Kong, China Fax: +852-26 35 00 75
There has been a dramatic increase in the incidence of adenocarcinoma of the distal esophagus in the last two decades. The culprit is Barrett's esophagus—intestinal metaplasia at the lower end of the esophagus as a result of acid reflux. Barrett's esophagus is not uncommon, being seen in approximately one in 100 endoscopic examinations and in 10-15% of patients with reflux esophagitis. Periodic endoscopic surveillance is suggested for this premalignant condition. Lifelong surveillance is fraught with difficulties, and is of questionable benefit in influencing survival. Surgical resection, although curative, carries appreciable morbidity and mortality.
Recently, interest has focused on endoscopic destruction of Barrett's mucosa with Nd: YAG or argon laser, photodynamic therapy, or multipolar electrocoagulation. If gastric acid is suppressed, the mucosal surface is often restored by squamous epithelium, with regression of the Barrett's mucosa.
Van Laethem and his colleagues at Erasmus Hospital in Brussels used endoscopic argon beam coagulation to obliterate Barrett's mucosa. The argon beam coagulator, which uses ionized argon gas to effect monopolar electrocoagulation in a non-contact manner, is suitable for mucosal obliteration, since the thermal damage is confined to a depth of 2-3 mm.
Thirty-one patients with Barrett's esophagus of at least 3 cm in length were treated. Argon beam coagulation was performed at monthly intervals, and patients required a mean of 2.4 sessions. On endoscopic examination, complete eradication was achieved in 25 of 31 patients (80.7%), although residual glands of intestinal metaplasia were found in six of the 25 on histological examination,
giving a success rate of only 61%. Complete eradication was more easily achieved in short Barrett segments and in non-circumferential lesions. Three complications occurred: one case of severe esophagitis and two esophageal stenoses. During the course of treatment, the patients received 40 mg of omeprazole daily and received either 40 mg or 10 mg of omeprazole on follow-up. Seventeen patients completed a one-year follow-up, and only nine were clear of metaplastic glands. Five of these patients took 10 mg omeprazole and four took 40 mg omeprazole daily.
Overholt and colleagues in Nashville, Tennessee used photodynamic therapy (PDT). Forty-eight hours after injection of the photosensitizer porfimer sodium (Photofrin), red light at 630 nm from an argon-pumped dye laser was shone into the area using a diffuser inserted through a special transparent centering balloon. All patients were treated with omeprazole 20 mg twice a day for the first three months, and then once a day. Patients were followed up at three-monthly intervals with endoscopy, using Lugol's iodine staining. Residual areas of Barrett's esophagus was destroyed using Nd:YAG laser treatment.
One hundred patients, including 13 with superficial cancer, were treated. The surface area of the Barrett's esophagus was reduced in all cases. An estimated 75-80% of Barrett's mucosa converted to squamous epithelium, with complete elimination of the Barrett's mucosa
in 43 patients. Dysplasia was eliminated in 78 patients. Ten of the 13 malignancies were ablated. Adverse effects included chest pain, dysphagia, atrial fibrillation, and pleural effusions. Esophageal strictures developed in 34 patients. During follow-up, two patients were found to have high-grade dysplasia under the cover of the new squamous epithelium 18 and 22 months after PDT, and another patient developed a subsquamous adenocarcinoma six months after PDT.
If the specialized columnar epithelium of Barrett's esophagus is obliterated and the area is reepithelialized with squamous mucosa, the risk of adenocarcinoma is theoretically removed. Endoscopic methods of local destruction are opening up exciting new opportunities for the therapeutic endoscopist. An important question that remains unanswered is the depth of injury necessary to obliterate all viable columnar cells, as persistent intestinal metaplasia underneath the neosquamous epithelium may progress to cancer. How best to nurture the new squamous epithelium is another problem. Follow-up data are preliminary, but suggest that maintenance treatment with proton-pump inhibitors may not be sufficient. Perhaps laparoscopic Nissen fundoplication after squamous reepithelialization is a better strategy.
четверг, 21 мая 2009 г.
Functional dyspepsia: unraveling the relation between symptoms and mechanisms PART3 (FINAL)

aritcle by G. Vantrappen
Corresponding address: G. Vantrappen, M.D. Department of Medicine University of Leuven ZU Gasthuisberg Herestraat 49 B-3000 Leuven Belgium
Tel.: +32-16-3442 25, fax: +32-16-3444 19
Visceral hypersensitivity and functional dyspepsia
The lack of a consistent relationship between many dyspeptic symptoms and putative physiological disturbances has led several investigators to study the role of alterations in visceral sensory perception in the pathophysiology of dyspeptic symptoms. Altered visceral sensory perception may be due to central or peripheral hypersensitivity to mechanical or chemical stimuli, but also to altered viscerosomatic referral patterns of central origin.
Several studies have demonstrated that many patients with functional dyspepsia have hypersensitivity to gastric distension (they experience discomfort and pain at lower distension volumes than normal subjects), and show altered viscerosomatic referral areas. Mertz et al. (1998) compared perceptual thresholds, viscerosomatic referral patterns, and psychological symptoms in 23 patients with functional dyspepsia, 10 with organic dyspepsia, and in 15 healthy control individuals.
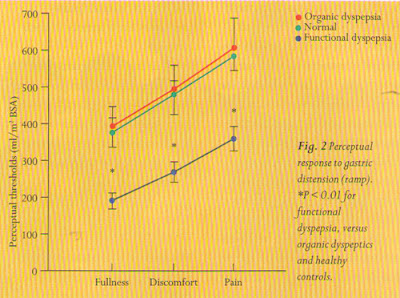
Patients with functional dyspepsia had clinical symptoms similar to those with organic dyspepsia (the prevalence of eight different clinical symptoms was similar in the two groups). However, only patients with functional disease reported hypersensitivity to gastric balloon distension: the volume thresholds for fullness, discomfort, and pain in response to slow gradual balloon distension were 40-50% lower in patients with functional dyspepsia than in those with organic causes or healthy volunteers. The thresholds in organic dyspeptics and healthy controls were similar (Fig. 2); 65% of functional dyspeptics and no patients with organic dyspepsia had hypersensitivity to distension. In addition, 52% of the functional dyspepsia patients showed altered viscerosomatic referral patterns, whereas only 20% of the organic disease patients experienced sensations in an aberrant location. Therefore, if abnormal sensation is defined as either aberrant referral or hypersensitivity to gastric distension, the sensitivity of abnormal sensation for functional dyspepsia is 87% and the specificity is 80%, when compared with an appropriate disease control.
There were no significant differences in psychological symptoms between functional and organic dyspeptics. Only the symptoms of severe nausea occurred more often in functional dyspepsia patients, and correlated with psychological distress, particularly anxiety.
In conclusion, these two papers on the relation between Symptoms and mechanisms of functional dyspepsia show that: a) impaired gastric accommodation to a meal has an important role in the generation of early satiety;
b) hypersensitivity to gastric distension, with lowered thresholds for fullness, discomfort, and pain, occurs only in patients with functional dyspepsia, not in organic dyspeptics.
вторник, 19 мая 2009 г.
Functional dyspepsia: unraveling the relation between symptoms and mechanisms PART2
aritcle by G. Vantrappen
Corresponding address: G. Vantrappen, M.D. Department of Medicine University of Leuven ZU Gasthuisberg Herestraat 49 B-3000 Leuven Belgium
Tel.: +32-16-3442 25, fax: +32-16-3444 19
Impaired gastric accommodation and early satiety
Tack et al. studied the role of impaired gastric accommodation to a meal in the production of early satiety—one of the symptoms of functional dyspepsia. Accommodation of the stomach to a meal consists of a relaxation
of the proximal stomach, providing the meal with a reservoir and allowing a volume increase without a rise in intragastric pressure. The authors hypothesized that impairment of gastric accommodation and reservoir function is likely to induce early satiety. They used a barostat to study postprandial fundus relaxation in 35 healthy subjects and in 40 functional dyspepsia patients. Gastric emptying, Helicobacter pylori status, sensitivity to gastric distension, and a dyspepsia symptom score were obtained from all patients. Eight different symptoms were evaluated: epigastric pain, bloating, postprandial fullness, early satiety, nausea, vomiting, belching, and epigastric burning. The amount of weight lost since the onset of symptoms was also noted. They found that impaired gastric accommodation to a

Fig. 1 Dyspepsia symproms in 40 consecutive patients withjunctional dyspepsia. Thefigure shows the number of patients grading individual symptoms as relevant or severe (score of> 2) in the subgroups with normal (MJ or impaired (U) gastric accomodation. Early satiety and weight loss of >S% of the initial body weight were significantly more prevalent in patients with impaired accomodation to a meal. Multivariate analysis showed that only early satiety was associated with impaired gastric accomodation.
meal was present in 16 of their 40 patients (40%). Impaired gastric accommodation was significantly associated with early satiety (Fig. 1), but not with the other dyspeptic symptoms. No correlation was present between impaired accommodation and other pathophysiological mechanisms, such as Helicobacter pylori gastritis, delayed gastric emptying, or hypersensitivity to gastric distension. The amplitude of the meal-induced satiety was correlated with the amount of calories the patients with early satiety had ingested at the time of maximum satiety. This observation also emphasizes the relation between impaired gastric accommodation and early satiety. The authors went one important step further and demonstrated that subcutaneous administration of a fundus-relax-ing drug (the 5-HTj receptor antagonist, sumatriptan) improves early satiety in their patients.
This is an important paper, for the first time demonstrating the causal relationship between early satiety and impaired gastric accommodation and pointing to possible ways of treating this symptom.
To be continued
четверг, 14 мая 2009 г.
Functional dyspepsia: unraveling the relation between symptoms and mechanisms PART1
aritcle by G. Vantrappen
Corresponding address: G. Vantrappen, M.D. Department of Medicine University of Leuven ZU Gasthuisberg Herestraat 49 B-3000 Leuven Belgium
Tel.: +32-16-3442 25, fax: +32-16-3444 19
Functional dyspepsia is a clinical syndrome defined by chronic or recurrent epigastric symptoms without identifiable cause when investigated by conventional means, including endoscopy with biopsies, radiology, and ultrasonography. The symptoms, which are assumed to be suggestive of upper gastrointestinal dysfunction, include fullness, discomfort and pain, early satietv, bloating and belching, and nausea and vomiting. The mechanisms thought to be involved in causing these symptoms include:
a) motility disturbances such as antral hypo-motility and delayed gastric emptying, gastric dysrhythmias,
and impaired gastric accommodation;
b) visceral hypersensitivity due to peripheral mechanisms such as enhanced sensitivity of afferent fibers, or due to central mechanisms such as central amplification of normal visceral input or increased vigilance towards expected painful stimuli; and
c) Helicobacter ■pylori gastritis.
A major problem with the concept of functional dyspepsia is the uncertainty about the relation between symptoms and functional disturbances. In some instances, this relation has been fairly well established, e.g. in the relation between heartburn and acid gastroesophageal reflux. Although all aspects of the relation have not been completely elucidated, there is little doubt that acid gastroesophageal reflux may lead to clinically relevant symptoms and esophagitis, and that treatment of acid reflux improves these symptoms and heals the lesions. Heartburn as a dominant symptom is therefore no longer considered to be part of the dyspepsia syndrome.
Two important papers were published in 1998 that shed new light on the relation between dyspeptic symptoms and physiological disturbances.
среда, 13 мая 2009 г.
Scientific News: Reflux Disorders

Article by Article by Eduardo G. Segal
Corresponding address: Eduardo Segal, M.D. Pueyrredn 60S - Piso 1 1032 Capital Federal Argentina
Fax: +54-1-961-9056
Although we are about to enter the new millennium, one of the major problems still to be solved in gastroenterology is that of gastroesophageal reflux disease (GERD), a condition that affects 40 million people in the United States alone.
Even though substantial advances have been made from the point of view of treatment, as well as in the pharmacological and surgical fields, we are still far from having heard the last word on the matter, since the pathogenesis of the disease is still uncertain. To date, transient lower esophageal sphincter (LES) relaxation, the control system of which may be located at the brain stem level, appears to be the most important mechanism for explaining reflux. However, drugs that might be able to inhibit initiation of LES relaxation are at present no more than possibilities for the future.
There is still controversy as to whether pharmacological or surgical treatment is preferable, and the two studies listed above are drawn from each of these fields. Surgeons have always taken part in round-table
discussions on the topic of GERD, and even before the advent of laparoscopic surgery, they participated in the treatment of patients with severe and refractory reflux episodes, or patients whose cases were complicated by stenosis refractory to endoscopic treatment, aspiration, or severe dysplasia. The recent advances in laparoscopic techniques for fundoplication, which are less invasive, have created renewed interest in the surgical field, and the leading proponents of these methods have been encouraging gastroenterologists' interest in them.
The laparoscopic focus of antireflux surgery now provides more acceptable options for the patient, with less postsurgical pain and a faster recovery. Frantzides and Richards last year published the largest series yet reported describing laparoscopic Nissen fundoplications. The series included 362 patients with GERD documented by radiography, endoscopy and/or pH surveillance during the 24 hours before surgery, who were followed up for a six-year period. The complication rate was 2% (n = 7), with no mortalities.
The postsurgical gastrointestinal symptoms were divided into two categories, those appearing within two months after surgery (Table 1), and those persisting for more than two months after surgery (Table 2).
Table 1 Laparoscopic Nissenjundoplication in the treatment of gastroesophageal reflux in 362 patients: gastrointestinal symptoms in the early postsurgical period (up to two months) (Frantzides and Richards, Surgery 1998; 124: 651-5).

Table 2 Laparoscopic Nissenfundoplication in the treatment of gastroesophageal reflux in 362 patients: gastrointestinal symptoms persistingfor more than two months (Frantzides and Richards, Surgery 1998; 124: 651-5).

As shown in Figure 1, lower esophageal sphincter pressure in patients before surgery (n = 58) was4± 1.2mmHg, and after surgery (n = 39) it was 14.6 +1.8 mmHg. As experience grew and the equipment used improved, the mean surgery time was reduced from 2.7 + 0.4 hours during the period 1991-94 to 1.8 (0.3 hours between 1994 and 1997. The hospitalization time required for the procedure decreased from 2.2 days in the first period to a mean of 1.5 days in the second. The authors conclude that, with strict selection criteria, increased experience and a standardized technique, laparoscopic Nissen fundoplication may provide safe and effective results for GERD patients.
Although pharmacological treatment has a high success rate (at least when there are no GERD complications), the length of the treatment time required has not yet been determined. This means that the costs of drug treatment are unpredictable—one of the arguments providing justification for the surgical approach. Eggleston et al. examined the cost-benefit ratio of medical treatment for GERD by analyzing cases included in a very large database, the Mediplus UK Database.
Figure 1. Lower esophageal sphincter pressure in patients before and after surgery. Presurgery pressure(n~ 58) of 4+ 1.2mmHg compared to postsurgery value (n = 39) of 14.6 ±1.8 mmHg.

The database was used to identify the health resources required during the first six months of treatment in three groups of patients initially prescribed cisapride, ranitidine, or omeprazole. Patients initially presenting with complicated GERD were excluded from the study.
The main strategies analyzed in previous studies have been those termed "step-up" and "step-down" treatments, used in the initial therapy for noncomplicated GERD. The step-up approach follows the principle of applying the minimum pharmacological effort necessary to achieve the therapeutic goal. The step-down approach, by contrast, suggests patients should be treated initially with a proton-pump inhibitor. The main problem inherent in the latter approach is the universal application of a powerful and expensive drug, even in patients in whom a minor intervention might suffice.
Table 3 Resource use and costs per 100 patients in the treatment of uncomplicated GERD in it. ■: Mediplus UK Database (Eggleston etal, Gut 1998; 42: 13-6).

Although the step-up approach was initially regarded as being the most effective option from the cost-benefit point of view, this view was not supported by the results of the study by Eggleston et al. The cost per patient for the initial six months of treatment based on therapy with cisapride, ranitidine, and omeprazole were £136, £177, and £189, respectively. All other results obtained from the analysis are presented in Table 3.
The study concludes that the step-up approach, starting with proki-netics or H 2-receptor antagonists, represents the initial therapeutic strategy with the higher cost-benefit ratio for the general practitioner treating a patient with an early diagnosis of non-complicated GERD.
Подписаться на:
Комментарии (Atom)